
Disclaimer: This blog is for informational and educational purposes only, intended for healthcare professionals and organizations. It does not constitute medical or professional advice. Full disclaimer here.
Purpose
This report highlights the growing care gap between Ontario’s retirement homes and long-term care (LTC) facilities, emphasizing the unique challenges and opportunities for for-profit retirement home operators.
1. Complex Care Needs in “Independent” Living:
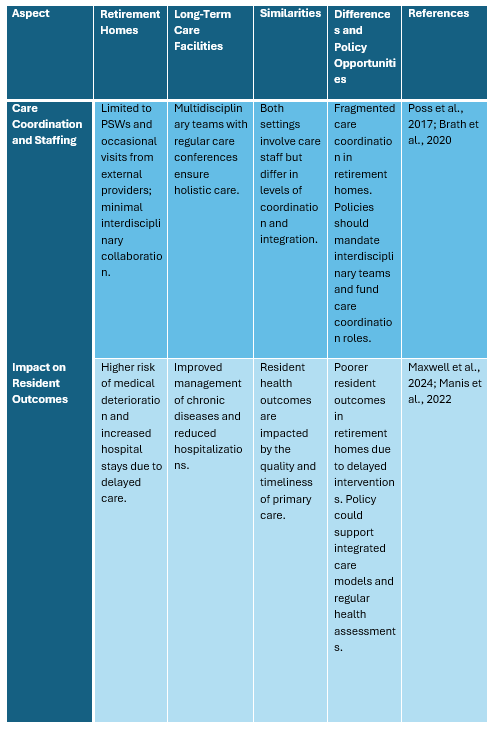
- Many retirement home residents have significant health needs, similar to LTC residents, yet lack consistent on-site medical support.
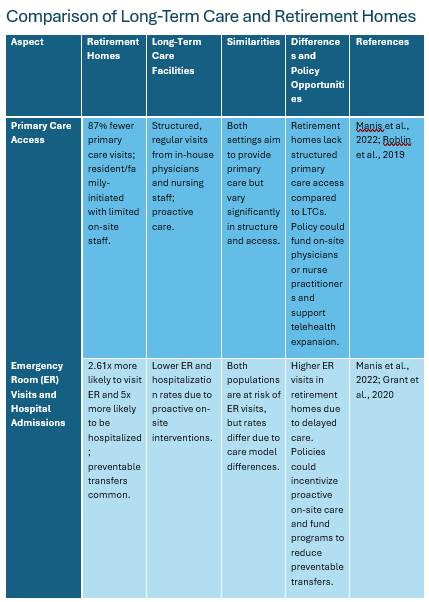
- Higher rates of ER visits and hospital admissions (2.6x and 5x higher, respectively) among retirement home residents highlight gaps in care delivery.
2. Profit vs. Quality – A False Dichotomy:
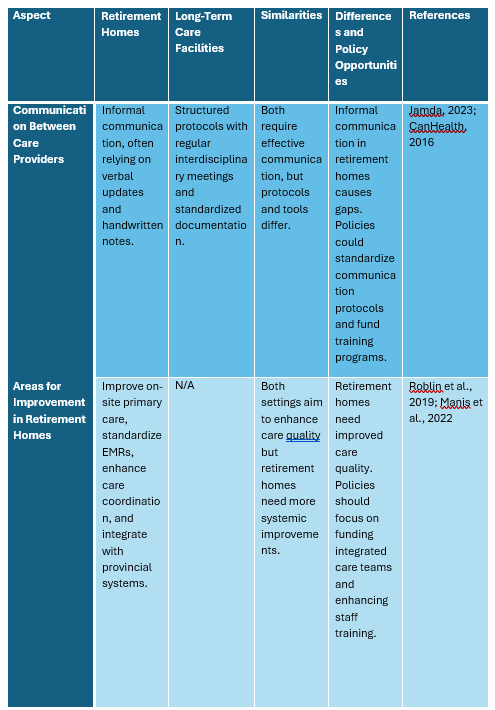
- Investing in quality care (on-site physicians, EMRs, interdisciplinary teams) can reduce ER transfers and improve resident outcomes.
- Enhanced care quality acts as a competitive advantage, attracting more residents and commanding premium pricing.
3. Policy Landscape:
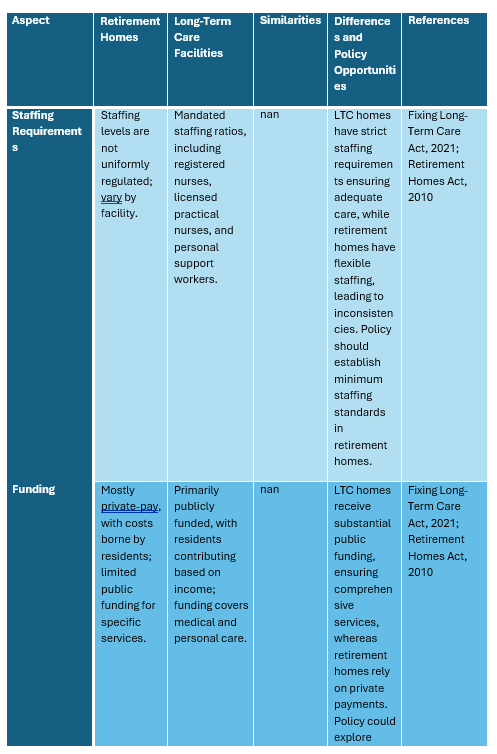
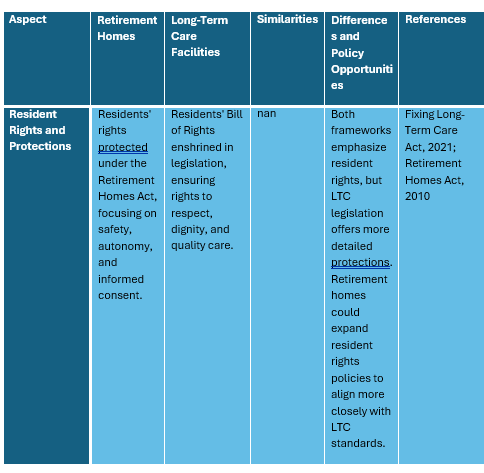
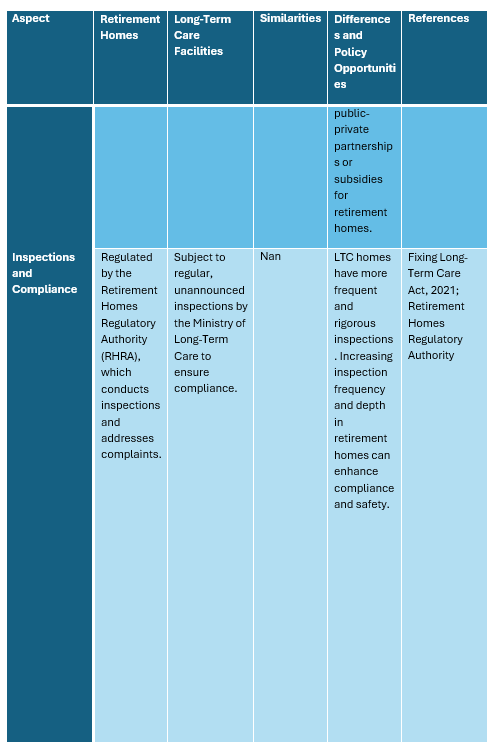
- LTC facilities operate under stricter regulations with mandated staffing ratios and public funding, whereas retirement homes rely heavily on private pay models with less oversight.
- Future policies may push for higher standards in retirement homes, creating an opportunity for forward-thinking operators to lead the market.
Strategic Recommendations:
- For Boards: Prioritize quality improvements as a means of driving occupancy and revenue growth.
- For Physicians: Champion proactive, interdisciplinary care to reduce preventable hospital visits.
- For Families: Encourage informed choices by evaluating the level of medical support provided.
- For Policymakers: Consider regulatory changes that promote equitable care standards across all elder care settings.
Why It Matters: Aligning profit goals with quality care isn’t just ethically responsible—it’s also a sustainable business strategy that strengthens reputation, enhances resident satisfaction, and ensures long-term success.


Prevalence and Resident Demographics in For-Profit Retirement Homes
Ontario is home to over 750 licensed retirement homes, the majority of which operate on a for-profit basis. In 2018, these homes collectively housed approximately 54,733 residents, with an average age of 86.7 years, and 69.0% being female. Common health conditions among residents include hypertension (86.2%), osteoarthritis (67.5%), mood disorders (63.9%), and dementia (37.7%).
Comparative Analysis: Retirement Homes vs. Long-Term Care Facilities
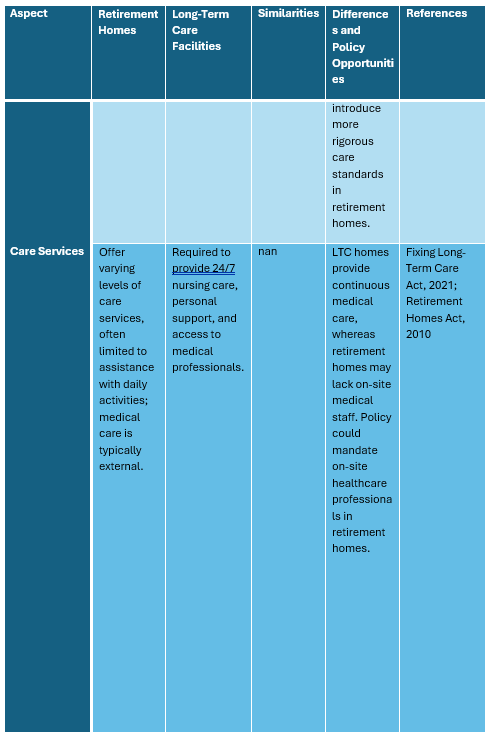
Long-term care (LTC) homes in Ontario differ significantly from retirement homes in terms of ownership, funding, and resident care needs. Of the 627 LTC homes, 57% are for-profit, 27% are not-for-profit, and 16% are publicly owned. Collectively, these facilities serve approximately 78,000 residents. Residents in LTC homes typically have more complex medical needs, necessitating 24-hour nursing care and assistance with most or all daily activities. In contrast, retirement homes are designed for seniors who are relatively independent but may require assistance with certain activities of daily living. However, a significant portion of retirement home residents—estimated at 40%—are long-stay home care patients, indicating substantial care needs that may approach those found in LTC settings.
The Misconception of ‘Independent Living’
The term ‘independent living’ associated with retirement homes can be misleading. Many residents require additional services due to prevalent health conditions such as hypertension, osteoarthritis, mood disorders, and dementia. This reality challenges the notion of complete independence and underscores the necessity for comprehensive care services within these facilities.
Health Service Utilization: Emergency Department Transfers and Hospital Admissions
Studies have highlighted notable differences in health service utilization between residents of retirement homes and those in LTC facilities. Residents of retirement homes have significantly higher rates of emergency department visits and hospital admissions compared to LTC residents. Specifically, per 1000 person-months, retirement home residents experience 10.62 emergency department visits and 5.42 hospital admissions, whereas LTC residents have 4.48 and 2.08 respectively. This disparity may stem from the lower availability of on-site medical and nursing care in retirement homes, leading to a reliance on external health services for acute medical issues.
Profit Motive vs. Quality of Care
Empirical evidence suggests a disparity in care quality between for-profit and not-for-profit LTC homes. Studies have found that for-profit facilities often deliver inferior care compared to their not-for-profit counterparts, attributed to fewer resources allocated to direct patient care, resulting in issues such as understaffing and higher incidences of health violations. This trend raises concerns about the impact of profit-driven models on resident well-being.
Financial Imperatives and Operational Challenges
For-profit retirement homes are accountable to stakeholders, necessitating a focus on profitability. This financial pressure can lead to cost-cutting measures that adversely affect care quality, such as reducing staffing levels or limiting investment in facility maintenance. The challenge lies in balancing fiscal responsibilities with the ethical obligation to provide high-quality care.
Quality as a Revenue-Enhancing Strategy
Contrary to the perception that quality improvement is inherently costly, enhancing care standards can serve as a differentiator in a competitive market, potentially leading to increased occupancy rates and revenue. For-profit corporations can adopt several strategies to achieve this balance:
Convincing Corporate Boards
To persuade boards of for-profit retirement home corporations to prioritize quality, it is essential to present a compelling business case: Market differentiation, risk mitigation, and long-term profitability are key arguments.
Critical Appraisal
While integrating quality improvement with profitability is theoretically sound, practical challenges persist. The initial investment required for staff development and facility upgrades may be substantial, and the return on investment may not be immediate. Additionally, systemic issues such as inadequate funding models and regulatory constraints can impede the implementation of quality-focused initiatives. Therefore, a multifaceted approach involving policy reform, stakeholder engagement, and a cultural shift within organizations is necessary to effect meaningful change.
Conclusion
The dichotomy between profit and quality in Ontario’s for-profit retirement homes presents a complex challenge. However, by recognizing quality care as a driver of financial success, these corporations can align their business objectives with the well-being of their residents. This alignment not only enhances the lives of seniors but also secures the long-term viability and reputation of the organizations.
Take home messages for Stakeholders
For Policy Makers:
“Bridging the Care Gap in Ontario’s Retirement Homes”
- Actionable Insight: Current regulations and funding mechanisms for retirement homes fall short in ensuring the same standard of care as long-term care (LTC) facilities, despite many residents having complex health needs.
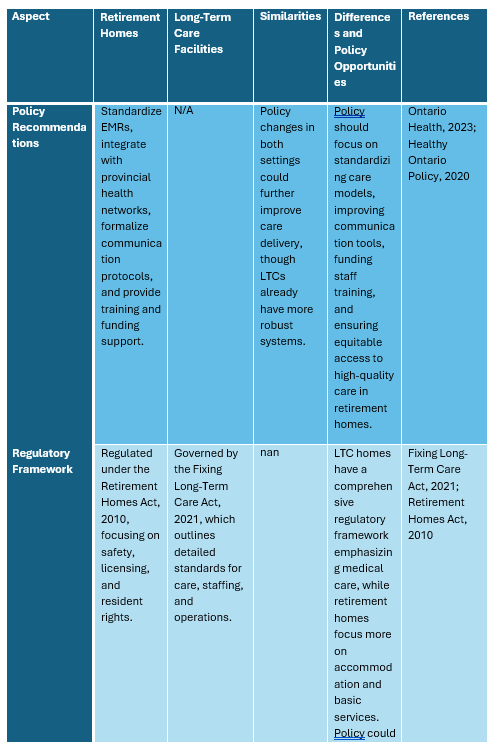
- Policy Opportunity: Implement standardized care protocols, fund on-site medical services, and mandate minimum staffing ratios in retirement homes to reduce preventable ER transfers and hospitalizations.
- Why It Matters: Enhancing regulatory oversight and aligning care standards across all senior living environments can improve health outcomes and reduce the burden on emergency services and hospitals.
For Retirement Home Boards:
“Quality Care as a Competitive Advantage”
- Key Message: Investing in quality care is not just ethically sound but also financially strategic. Facilities known for exceptional care attract more residents and command premium pricing.
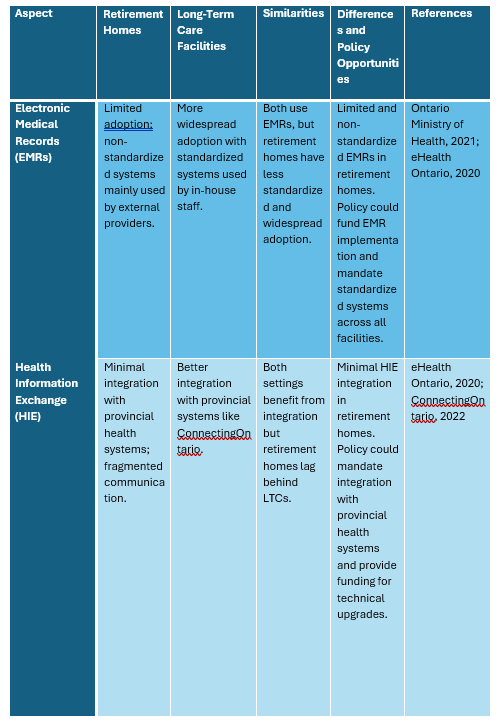
- Actionable Strategy: Employ on-site medical staff (e.g., nurse practitioners, physicians). Adopt standardized Electronic Medical Records (EMRs) to streamline care coordination. Prioritize staff training and interdisciplinary collaboration.
- Why It Matters: A commitment to high-quality care can differentiate your facility in a competitive market, leading to higher occupancy rates and long-term profitability.
For Physicians Working in Retirement Homes:
“Championing Integrated, Patient-Centered Care”
- Role Insight: Physicians play a pivotal role in reducing preventable ER transfers by advocating for on-site assessments, early interventions, and chronic disease management.
- Actionable Steps: Foster interdisciplinary collaboration among nurses, PSWs, and allied health staff. Utilize EMRs for comprehensive documentation and information sharing. Engage in proactive care planning with residents and families.
- Why It Matters: Physicians can directly impact residents’ quality of life by ensuring timely, continuous care, which reduces hospital visits and enhances patient satisfaction.
For Families Considering a Retirement Home:
“Choosing the Right Home for Your Loved One”
- Key Considerations: Not all retirement homes offer the same level of medical care. Understand the services provided, especially if your loved one has complex health needs.
- Questions to Ask: Is there on-site medical staff available? How are emergencies handled? What support exists for chronic conditions and daily living activities? How does the home ensure coordination with external healthcare providers?
- Why It Matters: Selecting a retirement home that aligns with your loved one’s health needs can significantly impact their well-being, safety, and quality of life.
References
Manis, D.R., Poss, J.W., Jones, A., et al. (2022). Rates of health services use among residents of retirement homes in Ontario: A population-based cohort study. CMAJ, 194, E730–E738.
Grant, K.L., Lee, D.D., Chen, I., et al. (2020). Reducing preventable patient transfers from long-term care facilities to emergency departments: A scoping review. CJEM, 22(6), 844–856.
Poss, J.W., Sinn, C.L.J., Crinchenko, G., et al. (2017). Location, Location, Location: Characteristics and Services of Long-Stay Home Care Recipients in Retirement Homes Compared to Others in Private Homes and Long-Term Care Homes. Healthcare Policy, 12(3), 80–93.
Maxwell, C.J., McArthur, E., Hogan, D.B., et al. (2024). Comparison of hospitalization events among residents of assisted living and nursing homes during COVID-19: Do settings respond differently during public health crises? PLoS One, 19(7), e0306569.
Ontario Ministry of Health (2021). Ontario Health Teams: Building a connected health care system. Retrieved from https://www.ontario.ca/page/ontario-health-teams
eHealth Ontario (2020). ConnectingOntario: Accessing comprehensive digital health information. Retrieved from https://www.ehealthontario.on.ca/en
Fixing Long-Term Care Act (2021). Government of Ontario. Retrieved from https://www.ontario.ca/laws/statute/21f39
Retirement Homes Act (2010). Government of Ontario. Retrieved from https://www.ontario.ca/laws/statute/10r11
Ontario Health (2023). Ontario Health’s plan for improving long-term care. Retrieved from https://www.ontariohealth.ca/
Healthy Ontario Policy (2020). Strategies for sustainable elder care in Ontario. Retrieved from https://www.ontario.ca/page/healthy-ontario